
If you run a health plan or sit in technical leadership at a managed care organization, publishing a credible FHIR implementation guide strategy has moved from a slow-burn priority to a hard deadline on your calendar. The work is no longer optional, the timelines from CMS are firm, and the operational consequences of falling behind on payer interoperability are getting more expensive every quarter.

This article walks through what these guides actually are, which ones matter most for payers right now, how the technical build looks in practice, what server and stack choices you face, and how to avoid the mistakes that quietly derail multi-year implementation programs.
An HL7 FHIR implementation guide is a structured specification that tells you exactly how to use the FHIR standard to solve a specific business problem. The base FHIR specification gives you a general framework with resources for patients, encounters, claims, coverage, and so on. But it intentionally leaves room for interpretation. That flexibility is good for generality and terrible for true interoperability since if your health plan uses one set of conventions and a hospital uses another, you cannot exchange records cleanly even when both technically conform to FHIR.
That is where FHIR implementation guides come in. They lock down the ambiguity: which fields are required, which value sets are permitted, how identifiers are structured, and what extensions are allowed. Think of the base FHIR specification as a language, and each implementation guide FHIR publishes as a grammar book for one specific conversation. For payers, multiple guides matter simultaneously because the conversations are different. Sharing records with members, with providers, and with other plans and processing prior authorizations all involve different resources, profiles, security models, and conformance expectations.
Healthcare software procurement teams at large U.S. health plans have been working through the CMS interoperability rules for years now, and the gap between intent and readiness is sobering. CMS finalized rule CMS-0057-F in January 2024, requiring impacted payers (Medicare Advantage organizations, state Medicaid and CHIP programs, Medicaid managed care plans, and Qualified Health Plan issuers on the Federally Facilitated Exchanges) to publish four FHIR-based APIs by January 1, 2027. Operational requirements like tightened decision turnarounds kick in even earlier, on January 1, 2026.
A successful FHIR implementation program is no longer a forward-looking R&D project. It is a regulated build with deadlines, audits, and public reporting on the other side. Here are a few numbers from credible sources that frame the urgency:
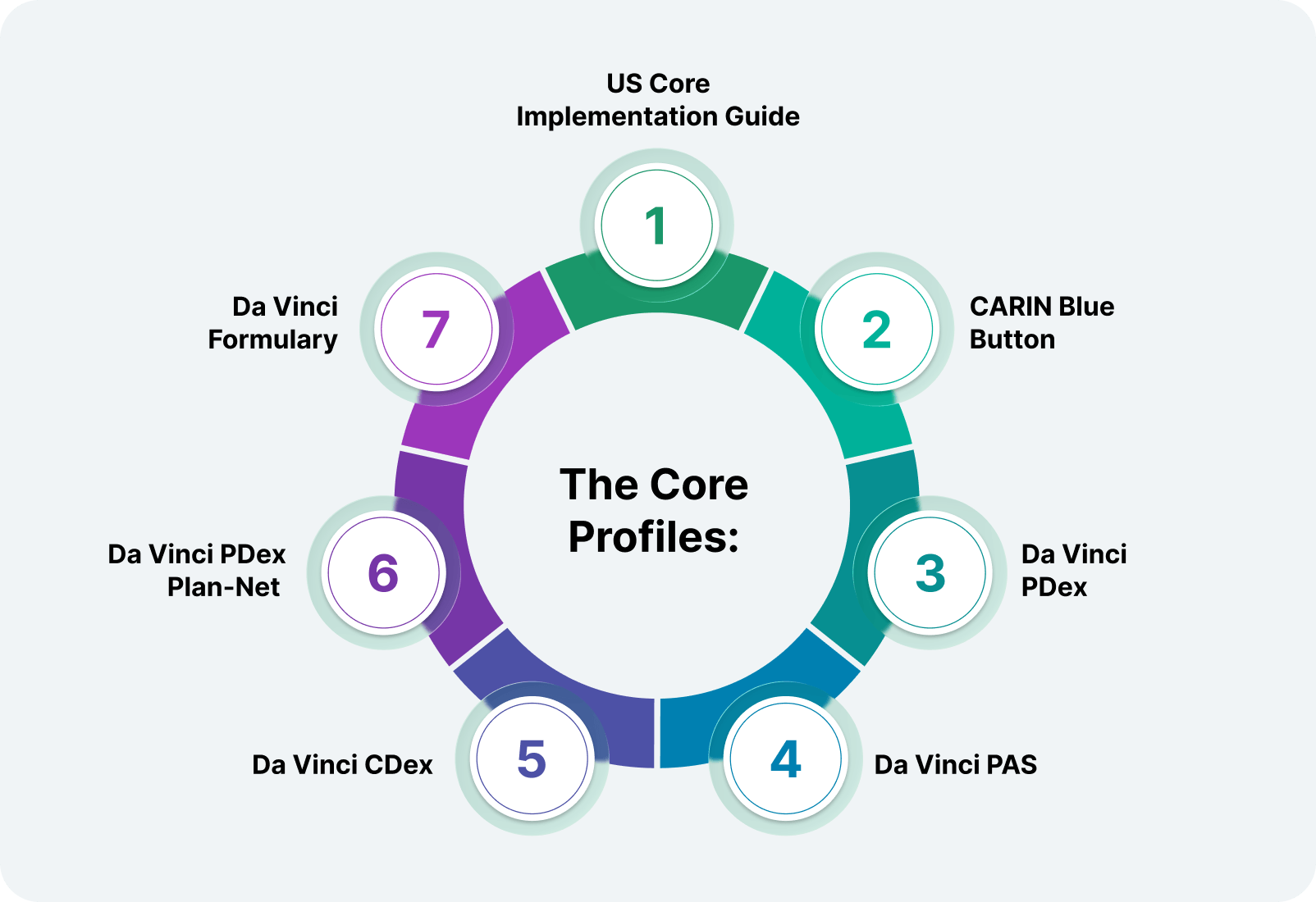
There is not one guide. There are several, and the ones a payer needs depend on which workflows are being digitized. Knowing which ones apply to your organization is the first real architectural decision in the program.
The FHIR US Core implementation guide is the foundational profile set for the United States. It defines minimum expectations for common resources (Patient, Practitioner, Observation, Condition, Medication Request, and others) so that systems across the country can exchange records with predictable structure. Most other US-focused IGs build on top of US Core rather than starting from raw FHIR. For a payer, US Core matters because nearly every clinical record you receive from a provider should already conform to it. If your inbound pipelines do not validate against US Core, you will quickly accumulate inconsistent records that cause problems downstream.
API healthcare integrations tend to surface this one early because CARIN Blue Button is the implementation guide behind the Patient Access mandate. It defines how member-facing apps retrieve claims, encounters, and explanation of benefits records from a health plan. If you are a CMS-impacted payer, your patient-facing endpoint needs to publish information conformant to this guide. The CMS Blue Button 2.0 program is the most visible production reference for it.
The HL7 Da Vinci Project produces most of the payer-facing guides you actually care about. PDex covers payer-to-payer member record exchange, the workflow where a new plan requests historical records from a member's previous plan after coverage starts. It defines how to share clinical resources, claims-derived records, and prior authorization history in a way the receiving payer can ingest cleanly.
PAS is the centerpiece of the technical build under CMS-0057-F. It defines how providers submit prior authorization requests electronically and how payers respond, whether by approval, denial with a specific clinical reason, or request for more information. The CMS FHIR API reference materials point heavily at PAS, and in practice it is paired with two other Da Vinci guides:
CDex covers payer-to-provider clinical record requests outside the prior authorization workflow. Risk adjustment record retrieval, medical record audits, quality measurement support, and HEDIS abstraction all run on CDex patterns.
The FHIR provider directory API is the technical face of Plan-Net. It defines how networks, locations, organizations, and practitioners are represented so that member-facing tools can show accurate, current network information. Maintaining directory accuracy has become its own compliance issue under federal No Surprises Act expectations, and Plan-Net is the standard that ties directory publishing to FHIR.
The formulary guide defines how plans publish drug coverage lists, including tier information, prior authorization flags, and step therapy rules. It powers member-facing tools that let people check whether a medication is covered before they fill a prescription, which directly reduces member service call volume.
People often get confused about the relationship between an implementation guide and an API. They are not the same thing, and conflating them tends to produce messy architecture decisions.
What is the FHIR API at its simplest? A FHIR API is a RESTful interface that lets clients read, write, search, and update FHIR resources over standard HTTPS. The implementation guide is the contract that specifies what those resources must look like to be valid. The API is the delivery mechanism. The guide is the spec it conforms to. Both are needed.
In payer terms, it is the actual server endpoint that providers, members, or other payers query to retrieve records. Practically, they are HTTP services that accept GET, POST, PUT, and DELETE requests against resource paths like /Patient/{id} or /Claim?patient={id} and return responses in JSON or XML. The FHIR API meaning is essentially "a healthcare REST API conformant to the FHIR specification, returning resources validated against one or more implementation guides."
A few quick definitions worth keeping straight:
A certified FHIR API is one that has passed conformance testing, usually through ONC certification programs or vendor-specific accreditation. For payers, certification matters because regulators expect verifiable conformance, not self-attestation. The FHIR APIs required under CMS-0057-F are four distinct endpoints: patient access, provider access, payer-to-payer, and prior authorization, each tied to specific implementation guides.
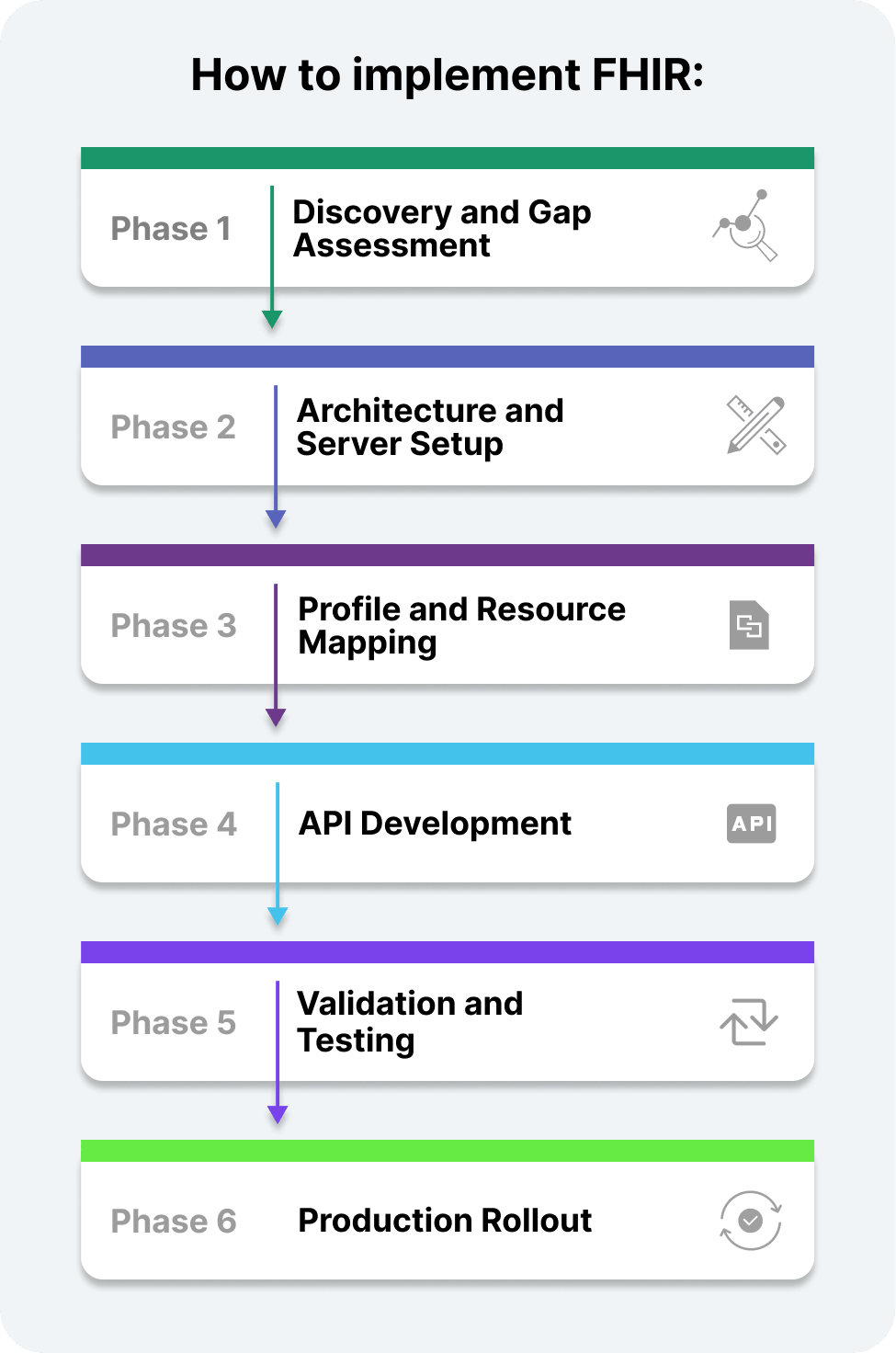
Integrating new technologies is not a weekend project, and it is not a single sprint. Serious FHIR implementations at the payer level run as multi-quarter programs with significant internal coordination across compliance, clinical operations, provider relations, and engineering. A mature HL7 FHIR implementation typically follows six phases.
Before architecting anything, audit what you have. What records do you hold, where, and in what format? Where are the gaps relative to US Core, CARIN, and the Da Vinci guides you need? What identity and consent infrastructure exists, and can it support member opt-in and opt-out at the resource level? This phase typically takes 6 to 12 weeks for a mid-sized payer. The output is a clear map of source systems, transformation requirements, and policy decisions that need to be made before any engineering starts.
A FHIR server implementation decision is one of the more consequential architecture choices in the entire program. Three managed-service paths dominate:
A fhir reference implementation like HAPI FHIR (Java) is widely used for both prototyping and for production. The HAPI project publishes its own FHIR Java API example patterns and a conformance test harness. For teams working in other stacks, the FHIR API Python ecosystem (fhirclient, fhir.resources) and FHIR .NET API options like the Firely .NET SDK are both mature and production-ready.
This is where you map your internal record models onto FHIR resources conformant to the relevant implementation guides. Each guide defines profiles, which are constrained versions of base resources with specific fields required, prohibited, or extended. For example, a claim record in your adjudication platform needs to map onto the FHIR patient API resource model plus ExplanationOfBenefit, Coverage, Encounter, and Practitioner resources, each conformant to CARIN profiles. This mapping work is where most engineering hours actually get spent and where most defects accumulate if it is rushed.
Custom product development teams typically build the API layer in parallel with the mapping work. The build itself follows familiar REST patterns: endpoints, OAuth 2.0 with healthcare-specific scopes for authentication, audit logging, and rate limiting. But conformance requirements are stricter than most general-purpose APIs.
To implement SMART on FHIR authentication, you need to support the SMART App Launch specification, which extends OAuth 2.0 with healthcare scopes like patient/Patient.read and launch contexts that pass clinical state from the EHR. The SMART on FHIR implementation guide is required reading for any team building the security model. A smart on FHIR API correctly implemented gives third-party app developers a standard, predictable way to integrate with your endpoints, which is the entire point of the pattern. HL7 FHIR APIs built to this convention are predictable to integrate against, which dramatically lowers the support burden once the API is live.
Serious FHIR API management requires automated conformance testing against every relevant profile, load testing against expected production volumes, and security testing against OWASP standards plus healthcare-specific threat models. Tools like Inferno (the ONC reference test suite), Touchstone, and the official HL7 FHIR Validator are essential.
For high-volume workloads, the bulk FHIR API specification (also called the FHIR Bulk Data API or FHIR Bulk Data Access IG) defines how to extract large populations of resources asynchronously. If your Provider Access API needs to serve millions of attributed members efficiently, single-resource fetches will not scale, and bulk export is the path.
Healthcare integration work rarely launches all at once. A phased rollout, starting with one product line, one region, or one set of provider partners, lets you find issues at a manageable scale before they become public regulatory events. Plan for a 60 to 90 day stabilization period before claiming production maturity, and treat the first 6 months of live operation as part of the build, not separate from it.

To make this concrete, here is a case for the Patient Access workflow that every CMS-impacted payer needs to support.
A member opens a third-party app, for instance, a health record consolidator like Apple Health or a chronic-condition management tool. The app initiates a SMART on FHIR authorization request to your FHIR patient access API. After the member authenticates and grants consent, the app receives an access token scoped to that member's records. The app then issues a series of FHIR REST requests:
Each response must conform to the relevant CARIN or US Core profile. A useful FHIR REST API example for end-to-end testing is the public CMS Blue Button 2.0 sandbox, which mirrors real production behavior for ExplanationOfBenefit and Coverage flows. This same patient access API FHIR pattern, with different scopes and resource types, underlies the Provider Access API and the Payer-to-Payer API. Build it cleanly once, and the additional endpoints become far more tractable.

Where you run your FHIR endpoints is one of the more consequential architecture decisions. Three broad paths exist: managed services (Azure, AWS, and Google), open-source reference servers (HAPI FHIR, Firely Spark, and Microsoft FHIR Server), and fully custom builds. Vendor APIs from EHR or established health IT players are not typically the right fit for payers since they are designed for providers, but they are worth knowing for context.
The athenahealth FHIR API is one such reference point on the provider side. The Cerner FHIR API (now Oracle Health) is another, with the Cerner FHIR API documentation publicly accessible and worth reviewing to see how a large EHR vendor publishes its conformance materials. Epic's FHIR endpoints round out the major provider-side references. For payers, these are useful comparison points, not direct procurement options.
For developers learning the territory, a practical FHIR API tutorial path is to start with the HAPI FHIR sandbox, then move to the HL7 FHIR specification documentation, then look at production FHIR API example code published by Firely, Microsoft, and the SMART Health IT project. The FHIR implementation guide registry at HL7.org lists every published IG with version history, which becomes essential reference material as the build progresses.
A solid FHIR implementation guide example to study before publishing your own is the CARIN Blue Button 2.0 IG. It is comprehensive, well-documented, and battle-tested across multiple payer production deployments. Reading it end-to-end is one of the more productive things a technical lead can do before kicking off architecture work.
When deciding which API for FHIR delivery to host on, weigh customization depth against operational cost. A managed FHIR healthcare API can ship faster than a custom build but caps your ability to inject custom logic at the resource validation layer. Choosing a FHIR-based API platform also affects how easily you can support emerging guides without vendor delays. An API FHIR endpoints require consistent operational practices regardless of the underlying platform: SLOs, monitoring, audit logging, and a real on-call rotation.

EMR system integration projects share many failure patterns with payer FHIR builds, and the lessons translate. Most FHIR-based APIs that miss their deadlines or ship unstable share a handful of avoidable mistakes:
AI voice assistant projects in healthcare and similar emerging tools often sit on top of FHIR endpoints, which means a FHIR API healthcare integration only works if the underlying FHIR layer is stable. Build the foundation well, or the application layer above it will struggle indefinitely. Understanding how to use fhir api workflows from the consumer side, not just the publisher side, is one of the more useful exercises for an architecture team. It surfaces conformance gaps that internal testing misses.
AI agents being deployed across healthcare workflows are increasingly used to monitor FHIR endpoint health, flag conformance regressions in real time, and surface anomalies in claims pipelines before they show up in public metrics. They do not replace good engineering practice, but they do reduce the operational burden of running production FHIR infrastructure.
Building a credible payer FHIR program is one of the more consequential infrastructure decisions a health plan will make this decade. Done well, it positions you for the next wave of regulatory expectations and gives you genuinely better operational visibility into how members interact with their coverage. Done poorly, you ship non-conformant endpoints, take regulatory heat, and end up rebuilding under time pressure with the rule already in effect.
EHR interoperability standards work has been moving steadily toward FHIR for years, and the regulatory layer has now caught up. The payers that treat this as a real engineering program (not a checkbox exercise) will come out the other side with infrastructure they can build on for the next decade. Those that wait will pay more for less.
If you are working through the planning decisions and want a partner that has done this kind of work before, our team specializes in FHIR integration & implementation services built around current U.S. regulatory requirements. We would be glad to walk through the specifics of your environment and help you build a roadmap that holds up under deadline pressure rather than collapses under it.

CTO & Technology Strategist
Andrei is the Chief Technology Officer at CleverDev Software, with deep expertise in software architecture, cybersecurity, cloud solutions, AI, and blockchain. He designs scalable, secure, and innovative systems that drive business growth. Known for blending technical excellence with strategic vision, Andrei leads teams in building future-ready digital solutions that deliver real value.

Our newsletter is packed with valuable insights, exclusive offers, and helpful resources that can help you grow your business and achieve your goals.


